
A lumbar disc bulge is one of the most common causes of lower back pain and sciatica.
Back pain is one of the leading causes of disability worldwide, but not every episode of back pain is caused by a “slipped disc.”
One of the most frequently reported findings on MRI scans is a lumbar disc bulge, yet many people who have a disc bulge never experience pain.
Quick Answer
A lumbar disc bulge occurs when one of the discs in your lower back extends beyond its normal boundary. It may cause lower back pain, sciatica, numbness, tingling, or muscle weakness if nearby nerves become irritated. Fortunately, most lumbar disc bulges improve without surgery through physiotherapy, targeted exercises, posture correction, staying active, and healthy lifestyle modifications. Early diagnosis and evidence-based rehabilitation can significantly speed recovery while reducing the risk of future episodes.
On the other hand, a relatively small bulge pressing on a sensitive nerve can cause severe pain, numbness, or weakness.
This difference often creates unnecessary fear.
Many people believe that once a disc bulges, surgery is inevitable or they should avoid all physical activity.
As physiotherapists, we know that this is rarely true.
Most lumbar disc bulges improve significantly with the right combination of education, movement, exercise therapy, posture correction, and lifestyle changes.
Recent research shows that remaining active, gradually strengthening the spine, and avoiding prolonged bed rest lead to better outcomes than complete inactivity.
In fact, many disc bulges naturally shrink over time as the body heals itself. (Brinjikji W, et al. AJNR)
Key Takeaways
- Most lumbar disc bulges improve successfully without surgery.
- MRI findings alone do not always explain back pain.
- Physiotherapy remains one of the most effective first-line treatments.
- Staying active usually promotes faster recovery than prolonged bed rest.
- Walking and core strengthening improve spinal support.
- Good posture and regular movement reduce pressure on spinal discs.
- Healthy body weight lowers stress on the lumbar spine.
- Proper lifting techniques help prevent future disc injuries.
- Seek urgent medical care if you develop bladder, bowel, or progressive leg weakness.
- Consistency with rehabilitation is the key to long-term recovery.
What Is a Lumbar Disc Bulge?
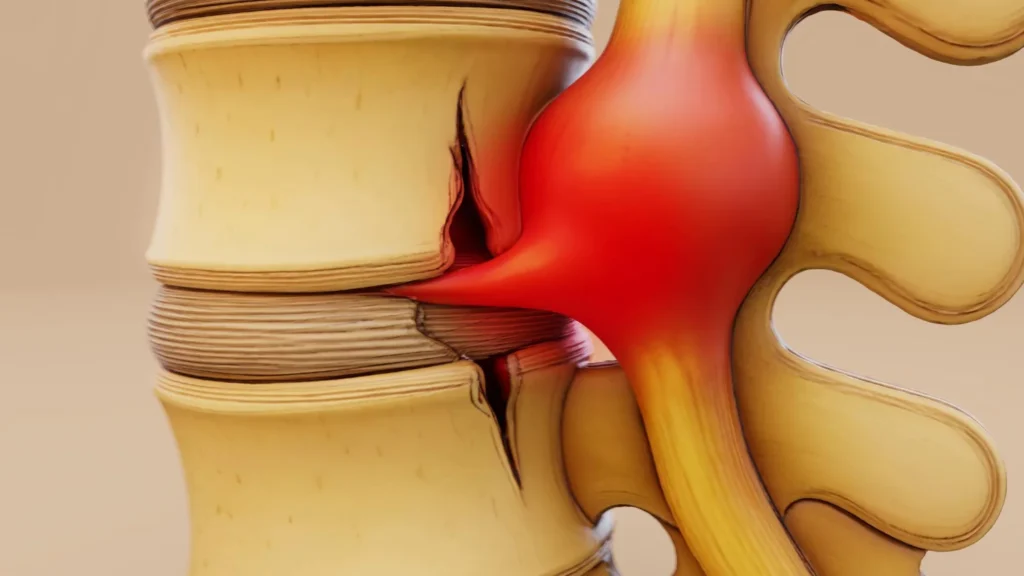
A lumbar disc bulge occurs when one of the cushioning discs between the bones of the lower back extends beyond its normal boundary.
Unlike a disc herniation, where the inner gel pushes through a tear in the outer layer, a disc bulge usually involves a broader outward extension of the disc without complete rupture.
Think of the disc as a jelly-filled doughnut.
With aging, repetitive stress, or injury, the outer ring weakens and begins to protrude outward.
This bulge may or may not compress nearby spinal nerves.
Importantly, a lumbar disc bulge is not always painful.
Studies have shown that disc bulges are commonly seen in people with no back pain at all.
Therefore, MRI findings should always be interpreted alongside symptoms and a physical examination rather than in isolation. (AJNR)
Understanding Your Lumbar Spine
Before discussing disc bulges, it helps to understand how your lower back works.
Vertebrae
The lumbar spine consists of five large vertebrae (L1 to L5).
These bones support most of your body weight and allow bending, lifting, and twisting.
Intervertebral Discs
Between every two vertebrae lies an intervertebral disc made up of:
- A tough outer ring called the annulus fibrosus
- A soft gel-like center called the nucleus pulposus
These discs function as shock absorbers during walking, running, lifting, and jumping.
Nerves
The spinal cord ends around the upper lumbar region, but nerve roots continue downward through the spinal canal before exiting toward the legs.
If a bulging disc irritates one of these nerves, symptoms such as sciatica can develop.
Muscles and Ligaments
Deep core muscles, multifidus, transverse abdominis, pelvic floor muscles, gluteal muscles, and spinal ligaments work together to stabilize the spine.
Weakness in these structures can increase stress on the lumbar discs over time. (Panjabi MM, PMC)
How Does a Lumbar Disc Bulge Develop?
Disc bulges usually develop gradually rather than suddenly.
During daily activities, discs repeatedly absorb pressure from:
- Sitting
- Standing
- Walking
- Lifting
- Twisting
- Sports
- Driving
Over years, the discs naturally lose water content and elasticity.
This age-related degeneration makes them less capable of distributing forces evenly.
Repetitive loading then causes the outer disc wall to stretch outward.
Sometimes a single heavy lifting incident can trigger symptoms, but in many individuals, the disc has been gradually weakening for years before pain appears.
Current evidence suggests that mechanical loading alone does not fully explain symptoms.
Inflammation around the affected nerve root also plays a significant role in causing pain. (Medline Plus)
Common Causes of Lumbar Disc Bulge
Age-Related Disc Degeneration
Natural aging remains the most common cause.
Disc hydration decreases progressively after the age of 30, reducing flexibility and increasing the risk of bulging.
Poor Lifting Technique
Repeated bending from the waist while lifting heavy objects increases pressure inside lumbar discs.
Physiotherapists often recommend:
- bending the knees
- keeping the load close
- engaging the core
- avoiding twisting while lifting
These simple modifications substantially reduce spinal stress.
Prolonged Sitting
Sitting for many hours increases disc pressure more than standing.
Office workers, truck drivers, gamers, and students often develop stiffness because prolonged sitting reduces movement, weakens postural muscles, and places sustained pressure on lumbar discs.
Changing positions every 30-45 minutes helps restore disc nutrition through movement. (The Waterside Practice)
Weak Core Muscles
The deep abdominal and spinal muscles function as the body’s natural back brace.
Weakness forces the passive structures, including discs and ligaments, to absorb more mechanical load during daily activities.
Research consistently supports exercise therapy as one of the most effective treatments for chronic low back disorders. (World Health Organisation)
Repetitive Twisting
Golf, tennis, cricket bowling, warehouse work, nursing, and manual labor often involve repeated rotational movements.
Over thousands of repetitions, these movements increase cumulative stress on lumbar discs.
Obesity
Extra body weight increases compressive forces across lumbar discs.
Interestingly, research also suggests obesity contributes through inflammatory pathways, not merely mechanical loading.
Weight management therefore benefits both spinal loading and inflammation. (Spine and Pain LA)
Smoking
Many people do not realize smoking accelerates disc degeneration.
Nicotine reduces blood flow to spinal tissues and impairs nutrient delivery to discs, slowing healing.
Smokers have significantly higher rates of lumbar degeneration and chronic back pain. (PubMed)
Risk Factors You Cannot Ignore
Although anyone can develop a lumbar disc bulge, certain factors increase the likelihood:
- Age over 30 years
- Sedentary lifestyle
- Long hours of sitting
- Repetitive heavy lifting
- Frequent bending and twisting
- Poor physical fitness
- Weak core muscles
- Smoking
- Obesity
- Previous back injury
- Family history of disc degeneration
Many of these risk factors are modifiable, which is encouraging because preventive physiotherapy can significantly reduce future episodes.
Symptoms of a Lumbar Disc Bulge
Symptoms vary depending on whether the bulging disc compresses nearby nerves.
Local Lower Back Pain
Many patients experience:
- dull aching pain
- stiffness
- muscle tightness
- pain after prolonged sitting
- discomfort while bending forward
Pain often fluctuates depending on activity levels.
Sciatica
If the disc irritates the sciatic nerve root, pain may travel from the lower back into the:
- buttock
- back of the thigh
- calf
- foot
This condition is commonly called sciatica.
Numbness and Tingling
Patients sometimes notice:
- pins and needles
- burning sensations
- reduced skin sensation
These symptoms usually follow the pathway of the affected nerve.
Muscle Weakness
More significant nerve compression can reduce strength in the:
- ankle
- foot
- toes
- calf muscles
Difficulty walking on the heels or toes should always be assessed promptly by a healthcare professional.
Pain That Changes Throughout the Day
One lesser-known feature of lumbar disc problems is that symptoms often fluctuate.
Many patients notice:
- worse pain in the morning
- stiffness after sitting
- improvement after gentle walking
- worsening after prolonged driving
Understanding these patterns helps physiotherapists tailor individualized rehabilitation programs.
Lesser-Known Facts About Lumbar Disc Bulges
Many Disc Bulges Heal Naturally
One fascinating discovery from modern imaging research is that the body can gradually reabsorb portions of bulging or herniated discs through natural inflammatory and immune mechanisms.
This explains why many patients improve substantially without surgery. (NCBI)
MRI Findings Do Not Always Match Pain
A surprising number of healthy adults have:
- disc bulges
- degeneration
- annular tears
without experiencing any symptoms whatsoever.
This is why physiotherapists assess movement, strength, nerve function, and symptom behavior rather than relying solely on MRI findings.
Walking Nourishes the Disc
Unlike many tissues, spinal discs have a very limited blood supply.
They receive nutrients through movement.
Gentle walking creates repeated compression and decompression cycles that help transport nutrients into the disc.
This is one reason complete bed rest is no longer recommended for most patients. (WHO Guidelines, 2023)
How a Physiotherapist Evaluates a Lumbar Disc Bulge
A physiotherapy assessment goes far beyond reviewing MRI reports.
We carefully evaluate:
Pain Characteristics
- location
- intensity
- duration
- aggravating factors
- relieving positions
Movement Assessment
Your physiotherapist observes how your spine responds to:
- bending
- extension
- side bending
- rotation
Sometimes a repeated movement actually reduces leg pain, providing valuable clues for treatment planning.
Neurological Examination
This includes testing:
- muscle strength
- tendon reflexes
- sensation
- nerve tension tests
These findings help determine whether nerve compression is present and how severe it may be.
Functional Assessment
Finally, we evaluate how your symptoms affect everyday life, including:
- walking
- sitting
- driving
- lifting
- work activities
- sleep
- exercise
Rather than treating the MRI alone, physiotherapy focuses on restoring confidence, improving movement quality, reducing pain, and helping patients safely return to normal activities.
How Is a Lumbar Disc Bulge Diagnosed?
One of the biggest misconceptions I see as a physiotherapist is that an MRI alone diagnoses the cause of back pain.
In reality, diagnosing a lumbar disc bulge requires combining your symptoms, physical examination, medical history, and imaging findings.
Many people have disc bulges visible on MRI yet experience no pain, while others with only a small bulge may have significant symptoms because the nearby nerve is irritated.
Healthcare professionals typically diagnose a lumbar disc bulge through a combination of:
- Detailed symptom history
- Physical examination
- Neurological assessment
- Functional movement testing
- Imaging (only when appropriate)
Current international guidelines recommend avoiding unnecessary imaging during the first few weeks of uncomplicated low back pain because it rarely changes treatment decisions and may increase anxiety.
Imaging is usually reserved for patients with severe neurological symptoms, suspected fractures, infection, cancer, or when surgery is being considered. (American College of Physicians)
Physical Examination
A physiotherapist’s assessment often provides more useful information than imaging alone.
During your examination, we evaluate:
Pain Pattern
Questions commonly include:
- Where exactly is the pain?
- Does it travel below the knee?
- What movements make it worse?
- What movements relieve it?
- Is the pain constant or intermittent?
These answers help determine whether the symptoms are more likely coming from the disc, muscles, joints, or nerves.
Range of Motion
We assess how comfortably you can:
- Bend forward
- Bend backward
- Lean sideways
- Rotate your trunk
Certain movement patterns may either increase or centralize symptoms, helping guide exercise selection.
Neurological Examination
A thorough neurological assessment includes checking:
- Muscle strength
- Reflexes
- Skin sensation
- Balance
- Walking pattern
Weakness, reduced reflexes, or altered sensation may suggest nerve root involvement requiring closer monitoring. (NICE Guideline)
Straight Leg Raise Test
One commonly used clinical test is the Straight Leg Raise (SLR).
During this test, the therapist gently lifts your straight leg while you lie on your back.
Pain radiating below the knee between approximately 30° and 70° of hip flexion may indicate irritation of the sciatic nerve caused by a lumbar disc bulge or disc herniation.
Although helpful, this test is only one piece of the overall clinical picture. (PMC)
Imaging Tests
MRI
MRI is considered the gold standard for visualizing soft tissues.
It clearly shows:
- Disc bulges
- Disc herniations
- Nerve compression
- Spinal canal narrowing
- Ligament injuries
However, MRI findings should never be interpreted in isolation because age-related disc changes are extremely common.
X-ray
X-rays cannot show discs.
Instead, they help identify:
- Fractures
- Alignment problems
- Arthritis
- Degenerative bone changes
An X-ray alone cannot confirm a lumbar disc bulge.
CT Scan
CT scans provide better bone detail than MRI but less soft tissue information.
They are usually reserved for patients who cannot undergo MRI or when detailed bone imaging is required.
Can a Lumbar Disc Bulge Heal Naturally?
One of the most reassuring facts for patients is that yes, many lumbar disc bulges improve naturally over time.
The human body has an impressive ability to reduce inflammation, absorb damaged disc material, and adapt surrounding tissues.
Research has demonstrated spontaneous regression of many lumbar disc protrusions and herniations through immune-mediated processes.
This explains why many patients recover without injections or surgery. (MDPI)
As physiotherapists, our goal is to support this natural healing process by:
- Reducing unnecessary stress on the spine
- Improving movement quality
- Strengthening supporting muscles
- Restoring confidence in movement
Physiotherapy Treatment for Lumbar Disc Bulge
Physiotherapy is considered one of the first-line treatments for most lumbar disc bulges.
Treatment is individualized because every patient’s symptoms, lifestyle, occupation, and goals are different.
Patient Education
Surprisingly, one of the most powerful treatments is education.
Understanding that:
- discs can heal
- pain does not always equal damage
- movement is generally safe
helps reduce fear, improve confidence, and encourage early recovery.
Modern pain science consistently shows that reassurance and education improve outcomes.
Activity Modification
Complete bed rest was once commonly prescribed.
Today, evidence strongly discourages prolonged bed rest because it leads to:
- muscle weakness
- joint stiffness
- slower recovery
- reduced confidence
- poorer long-term outcomes
Instead, patients are encouraged to remain as active as symptoms allow.
Gentle movement promotes circulation, nourishes spinal discs, and maintains muscle function.
Therapeutic Exercise
Exercise is the cornerstone of physiotherapy management.
The right exercises help:
- improve spinal stability
- reduce pain
- strengthen muscles
- restore flexibility
- improve endurance
- prevent recurrence
International guidelines consistently recommend exercise therapy as a primary treatment for persistent low back pain.
McKenzie Method (Mechanical Diagnosis and Therapy)
The McKenzie Method is widely used in physiotherapy for disc-related back pain.
It involves repeated spinal movements that may help “centralize” symptoms.
Centralization means leg pain gradually moves back toward the lower back, which is generally considered a positive sign.
Not every patient responds to McKenzie exercises, but for appropriately selected individuals, they can provide significant relief. (PubMed)
Core Strengthening
Your spine depends on muscular support just as much as it depends on bones and discs.
Important stabilizing muscles include:
- Transverse abdominis
- Multifidus
- Diaphragm
- Pelvic floor
- Obliques
- Gluteal muscles
Rather than performing endless sit-ups, physiotherapists focus on controlled stabilization exercises that improve coordination and endurance.
Examples include:
- Abdominal bracing
- Bird Dog
- Dead Bug
- Modified Side Plank
- Glute Bridge
- Pallof Press
Research consistently supports motor control exercises for improving pain and function in people with chronic low back pain. (NLM)
Flexibility Training
Tight muscles often increase stress on the lumbar spine.
Your physiotherapist may prescribe stretching for:
- Hamstrings
- Hip flexors
- Piriformis
- Gluteals
- Calves
Stretching should always be individualized because aggressive stretching during acute nerve irritation can temporarily worsen symptoms.
Walking Program
Walking remains one of the safest and most effective exercises for many people with lumbar disc bulges.
Benefits include:
- Better blood circulation
- Improved disc nutrition
- Reduced stiffness
- Improved endurance
- Enhanced mood
- Weight management
Most patients tolerate several short walks better than one long walk.
Manual Therapy
Hands-on physiotherapy techniques may include:
- Joint mobilization
- Soft tissue release
- Myofascial techniques
- Gentle spinal mobilization
Manual therapy is generally most effective when combined with active exercise rather than used as a standalone treatment.
Dry Needling
Some physiotherapists use dry needling to reduce muscle tightness around the lumbar spine.
While dry needling may help decrease muscle pain in selected patients, it does not correct the disc bulge itself.
Current evidence suggests it can be useful as part of a comprehensive rehabilitation program rather than as the primary treatment.
Heat Therapy
Heat can help reduce:
- Muscle spasm
- Stiffness
- Pain
Warm packs are often useful before stretching or exercise sessions.
Ice Therapy
Ice is generally more helpful during the early inflammatory stage following an acute injury.
Apply for approximately 10-15 minutes with a protective towel to avoid skin injury.
Electrical Stimulation (TENS)
Transcutaneous Electrical Nerve Stimulation (TENS) may temporarily reduce pain for some individuals.
However, current evidence suggests that TENS should not replace exercise-based rehabilitation and education.
It may be considered an adjunct rather than a primary treatment.
Lumbar Traction: Does It Really Work?
Traction has been used for decades, but research findings are mixed.
Some patients experience short-term symptom relief, particularly those with specific nerve root compression patterns.
However, current clinical guidelines do not recommend routine traction for all patients because long-term benefits remain uncertain.
If traction is used, it should be carefully selected and combined with active rehabilitation rather than relied upon as a standalone therapy.
Medications
Doctors may recommend medications alongside physiotherapy, including:
- Acetaminophen (in selected cases)
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Muscle relaxants (short-term)
- Neuropathic pain medications for nerve-related symptoms
Medication should always be taken under medical supervision due to potential side effects and contraindications.
Epidural Steroid Injections
For patients with persistent nerve pain that does not improve with conservative care, epidural steroid injections may reduce inflammation around the affected nerve root.
These injections may provide temporary symptom relief, allowing patients to participate more effectively in physiotherapy.
They do not repair the disc itself and are not necessary for most people.
When Is Surgery Needed?
Fortunately, only a small percentage of patients with lumbar disc bulges require surgery.
Surgical consultation may be considered if there is:
- Progressive muscle weakness
- Loss of bladder or bowel control
- Cauda equina syndrome
- Severe, persistent leg pain despite adequate conservative treatment
- Significant neurological deficits confirmed clinically and on imaging
Even when surgery is indicated, postoperative physiotherapy remains essential for restoring strength, flexibility, and function.
Lesser-Known Tips That Can Speed Recovery
Many people overlook these simple but effective strategies:
Change Positions Frequently
Remaining in one posture for long periods increases disc pressure.
Aim to change your position every 30-45 minutes.
Walk Before Stretching
A short five-minute walk warms up muscles and often makes stretching more comfortable and effective.
Avoid Holding Your Breath While Lifting
Breathing normally while engaging your core reduces unnecessary spinal pressure.
Improve Hip Mobility
Limited hip movement forces the lower back to compensate during bending and twisting.
Maintaining healthy hip flexibility can reduce lumbar strain.
Sleep Is a Powerful Healing Tool
Disc tissue recovery and overall healing are influenced by sleep quality.
Aim for 7–9 hours of restorative sleep each night to support tissue repair and pain modulation.
Best Sleeping Positions for a Lumbar Disc Bulge
Sleep is one of the most overlooked components of recovery.
During sleep, your muscles relax, inflammation decreases, and damaged tissues begin repairing themselves.
However, an unsupported sleeping position can place unnecessary stress on the lumbar spine and aggravate symptoms the following morning.
Sleeping on Your Back
For many people, sleeping on the back is the most comfortable position.
Place a pillow under your knees to slightly bend the hips and knees.
This helps flatten the natural arch in the lower back, reducing pressure on the lumbar discs.
A medium-firm mattress generally provides adequate support while allowing the spine to maintain a neutral position.
Sleeping on Your Side
Side sleeping is often recommended for people with sciatica caused by a lumbar disc bulge.
Place a pillow between your knees to keep your pelvis level and reduce twisting of the lower back.
Try to keep your hips and knees slightly bent rather than curled tightly into a fetal position.
Sleeping on Your Stomach
This position is usually the least favorable because it increases lumbar extension and places the neck in prolonged rotation.
If you cannot avoid sleeping on your stomach, placing a thin pillow beneath your pelvis may reduce stress on the lower back.
Sleep position recommendations for spinal pain are supported by ergonomic and musculoskeletal research emphasizing maintenance of a neutral spine during rest. (NCBI)
Sitting Posture and Workstation Ergonomics
As physiotherapists, one of the first questions we ask is, “How many hours do you sit each day?”
Modern lifestyles often involve prolonged sitting, which increases pressure within the lumbar discs more than standing or walking.
Maintain a Neutral Spine
While in sitting posture:
- Keep both feet flat on the floor.
- Knees should remain approximately at hip level.
- Sit with your hips positioned fully back in the chair.
- Relax your shoulders.
- Keep your ears aligned with your shoulders instead of leaning your head forward.
Avoid slouching, as it increases stress on the lower back and surrounding soft tissues.
Use Lumbar Support
A small lumbar roll or an ergonomically designed chair can help maintain the natural curve of your lower back during prolonged sitting.
Follow the 30-30 Rule
One of the simplest strategies I recommend to patients is the 30-30 Rule.
Every 30 minutes, stand up and move for at least 30-60 seconds.
Walk around, stretch gently, or simply change your position.
This movement restores circulation, reduces stiffness, and decreases prolonged disc loading.
Optimize Your Computer Setup
Your monitor should be positioned at eye level.
Keep the keyboard close enough that your elbows remain at approximately 90 degrees.
Avoid leaning toward your screen, especially while working on laptops for extended periods.
Things You Should Do
Recovering from a lumbar disc bulge is not about complete rest. It is about smart movement.
Stay Physically Active
Gentle movement improves circulation, reduces stiffness, and helps maintain muscle strength.
Activities that are often well tolerated include:
- Walking
- Swimming
- Stationary cycling (if comfortable)
- Guided physiotherapy exercises
Strengthen Your Core
A strong core reduces unnecessary stress on the lumbar discs.
Your rehabilitation should gradually strengthen:
- Deep abdominal muscles
- Multifidus
- Gluteal muscles
- Hip muscles
- Pelvic floor
Maintain a Healthy Weight
Even a modest reduction in body weight can decrease the mechanical load placed on the lumbar spine.
Warm Up Before Exercise
Cold muscles are less flexible and more susceptible to injury.
Spend five to ten minutes performing gentle walking or mobility exercises before exercising.
Lift Correctly
Whenever lifting:
- Bend at the hips and knees.
- Keep the object close to your body.
- Tighten your core.
- Avoid twisting while carrying weight.
Things You Should Avoid
Many daily habits unknowingly delay recovery.
Avoid:
- Prolonged bed rest
- Sitting continuously for several hours
- Heavy lifting during acute pain
- Sudden twisting movements
- Repeated forward bending without control
- High-impact activities if symptoms worsen
- Ignoring persistent numbness or weakness
- Smoking
One lesser-known mistake is repeatedly testing your pain by bending forward every few minutes.
Constantly provoking symptoms may irritate already sensitive tissues and slow recovery.
Can Exercise Make a Disc Bulge Worse?
Patients frequently ask this question.
The answer depends on which exercise, how it is performed, and whether it is appropriate for your stage of recovery.
Research consistently shows that appropriately prescribed exercise is beneficial rather than harmful for most people with lumbar disc bulges.
However, exercises performed with poor technique or progressed too quickly may temporarily aggravate symptoms.
This is why individualized physiotherapy is so valuable.
Nutrition for Spinal Health
Although no specific food can “heal” a disc bulge, a nutrient-rich diet supports tissue repair and helps reduce chronic inflammation.
Focus on:
Protein
Supports muscle recovery and tissue repair.
Good sources include:
- Eggs
- Fish
- Chicken
- Lentils
- Greek yogurt
- Tofu
Omega-3 Fatty Acids
May help reduce inflammation.
Sources include:
- Salmon
- Sardines
- Walnuts
- Flaxseeds
- Chia seeds
Calcium and Vitamin D
Essential for maintaining healthy bones that support the spine.
Magnesium
Supports muscle relaxation and normal nerve function.
Found in:
- Pumpkin seeds
- Almonds
- Spinach
- Beans
Stay Hydrated
Intervertebral discs contain a high percentage of water.
While drinking extra water does not “reinflate” a damaged disc, maintaining adequate hydration supports overall tissue health and normal physiological function.
Recovery Timeline
Every patient heals differently.
A general timeline is:
First 2 Weeks
- Pain control
- Gentle walking
- Activity modification
- Education
- Light mobility exercises
Weeks 2 to 6
- Progressive strengthening
- Improved flexibility
- Reduced nerve irritation
- Increased daily activity
Weeks 6 to 12
Many patients notice substantial improvement in:
- Walking tolerance
- Sitting tolerance
- Strength
- Confidence
- Return to work
Three Months and Beyond
The focus shifts toward:
- Preventing recurrence
- Building resilience
- Returning to sports
- Long-term exercise habits
Some individuals recover sooner, while others with severe nerve compression may require a longer rehabilitation program.
When Should You Seek Immediate Medical Attention?
Although most lumbar disc bulges improve with conservative care, certain symptoms require urgent medical evaluation.
Seek immediate medical attention if you develop:
- Loss of bladder or bowel control
- Numbness around the groin or saddle area
- Progressive weakness in one or both legs
- Severe pain following significant trauma
- Fever accompanied by severe back pain
- Unexplained weight loss with persistent back pain
- History of cancer with new-onset back pain
- Pain that is constant, severe, and unrelated to movement
These may indicate serious conditions requiring urgent assessment.
My Clinical Insight
One of the biggest mistakes I see in clinical practice is that patients become frightened after reading their MRI report.
The words disc bulge, degeneration, or disc protrusion often sound alarming, but these findings are common and frequently occur even in people without pain.
Rather than focusing solely on imaging, I encourage my patients to focus on how their body functions.
Your ability to move comfortably, regain strength, improve flexibility, and confidently return to daily activities is often far more important than what appears on an MRI scan.
Recovery is rarely about finding a “magic exercise.”
It is about consistently following a structured rehabilitation program, improving posture, strengthening the muscles that support your spine, maintaining a healthy lifestyle, and gradually increasing activity.
Small improvements repeated every day usually produce the best long-term results.
Physio Prescription
As a physiotherapist, my practical advice for patients with a lumbar disc bulge is simple:
- Keep moving unless advised otherwise by your healthcare provider.
- Walk every day within your comfort level.
- Perform your prescribed exercises consistently rather than intensely.
- Strengthen your core and hip muscles.
- Change your sitting position frequently.
- Lift objects with proper technique.
- Sleep in a position that supports a neutral spine.
- Maintain a healthy body weight.
- Do not let fear of movement delay your recovery.
Remember, rehabilitation is a journey, not a race. Consistency almost always outperforms intensity.
Myth vs Reality
Myth: A lumbar disc bulge always causes pain.
Reality: Many people have lumbar disc bulges without experiencing any symptoms at all.
Myth: Surgery is the only solution.
Reality: Most people recover successfully with conservative management, including physiotherapy, education, and exercise.
Myth: Complete bed rest is best.
Reality: Prolonged bed rest often delays recovery. Gentle, appropriate movement is generally recommended.
Myth: Once a disc bulges, it never improves.
Reality: Research shows that many disc bulges and herniations partially regress over time through natural healing mechanisms.
Myth: Pain always means more damage.
Reality: Pain is influenced by multiple factors, including inflammation, nerve sensitivity, stress, sleep, and physical conditioning, not just structural changes.
Final Word
A lumbar disc bulge can certainly be painful, but it is not a life sentence.
Modern research has transformed our understanding of disc-related back pain.
We now know that most people improve with evidence-based conservative care, particularly when they stay active, participate in a structured physiotherapy program, and gradually rebuild strength and confidence.
Instead of fearing movement or relying solely on imaging findings, focus on improving the factors you can control: posture, physical activity, muscle strength, sleep quality, body weight, and overall health.
With patience, consistency, and the right guidance, many individuals return to work, sports, and daily life without surgery.
Frequently Asked Questions
1. Can a lumbar disc bulge heal on its own?
Yes. Many lumbar disc bulges gradually improve through the body’s natural healing process, especially when combined with physiotherapy and regular exercise.
2. Is walking good for a lumbar disc bulge?
Yes. Walking improves circulation, reduces stiffness, nourishes spinal discs, and helps maintain muscle strength.
3. Can I exercise with a lumbar disc bulge?
Yes, but exercises should be prescribed by a physiotherapist based on your symptoms and stage of recovery.
4. Is surgery always necessary?
No. Most people recover successfully with conservative treatment, including physiotherapy and lifestyle modifications.
5. How long does recovery usually take?
Many people notice significant improvement within 6 to 12 weeks, although recovery varies between individuals.
6. Which sleeping position is best?
Sleeping on your back with a pillow under your knees or on your side with a pillow between your knees is generally recommended.
7. Can sitting make a lumbar disc bulge worse?
Prolonged sitting increases disc pressure and may aggravate symptoms. Changing positions every 30 to 45 minutes is recommended.
8. Does a lumbar disc bulge always cause sciatica?
No. Many disc bulges cause only local back pain or no symptoms at all.
9. Can I lift weights after recovery?
Yes. Most patients can safely return to strength training after appropriate rehabilitation and guidance from a healthcare professional.
10. How can I prevent another lumbar disc bulge?
Maintain good posture, strengthen your core, stay physically active, lift correctly, manage your weight, and avoid prolonged sitting.
More Read






Medical Disclaimer!
This article has been reviewed and written under the guidance of our Head Physiotherapist, Dr. Kruti Raj (PT, MUHS,CPT,CMPT). The information shared is intended for educational purposes only and should not be considered a substitute for personalized medical advice, diagnosis, or treatment.
Please consult us or any other qualified healthcare professional before beginning any exercise program, especially if you are experiencing pain, recovering from injury, or managing a medical condition.



