
Bulging Disc vs Herniated Disc is one of the most confusing spine topics.
Knowing the difference can help you better understand your MRI results, choose the right treatment, and avoid unnecessary worry.
When patients walk into my clinic carrying an MRI report, one of the first questions they ask is,
“Doctor, is a bulging disc the same as a herniated disc?”
The short answer is no.
Although these terms are often used interchangeably, they describe two different stages of disc damage.
Understanding the difference can help you make informed treatment decisions and avoid unnecessary fear.
Quick Answer
A bulging disc occurs when the spinal disc extends outward but its outer layer remains intact. A herniated disc happens when the tough outer layer tears, allowing the soft inner material to leak out and potentially compress nearby nerves. While both conditions can cause back or neck pain, herniated discs are more likely to produce leg pain, arm pain, numbness, tingling, or muscle weakness. Fortunately, many patients improve with physiotherapy, exercise, and lifestyle changes without requiring surgery.
As a physiotherapist, I often reassure patients that an MRI finding does not always match the amount of pain they feel.
In fact, many healthy adults who have no back pain at all show bulging or even herniated discs on MRI scans.
This highlights why treatment should focus on your symptoms and physical examination, not imaging alone.
Research consistently shows that imaging findings should always be interpreted alongside the patient’s clinical presentation. (PubMed)
Key Takeaways
- A bulging disc is not the same as a herniated disc.
- Many bulging discs cause no symptoms.
- Herniated discs are more likely to irritate spinal nerves.
- MRI findings alone do not determine treatment.
- Physiotherapy is the first-line treatment for most patients.
- Most people recover without surgery.
- Movement is usually better than prolonged bed rest.
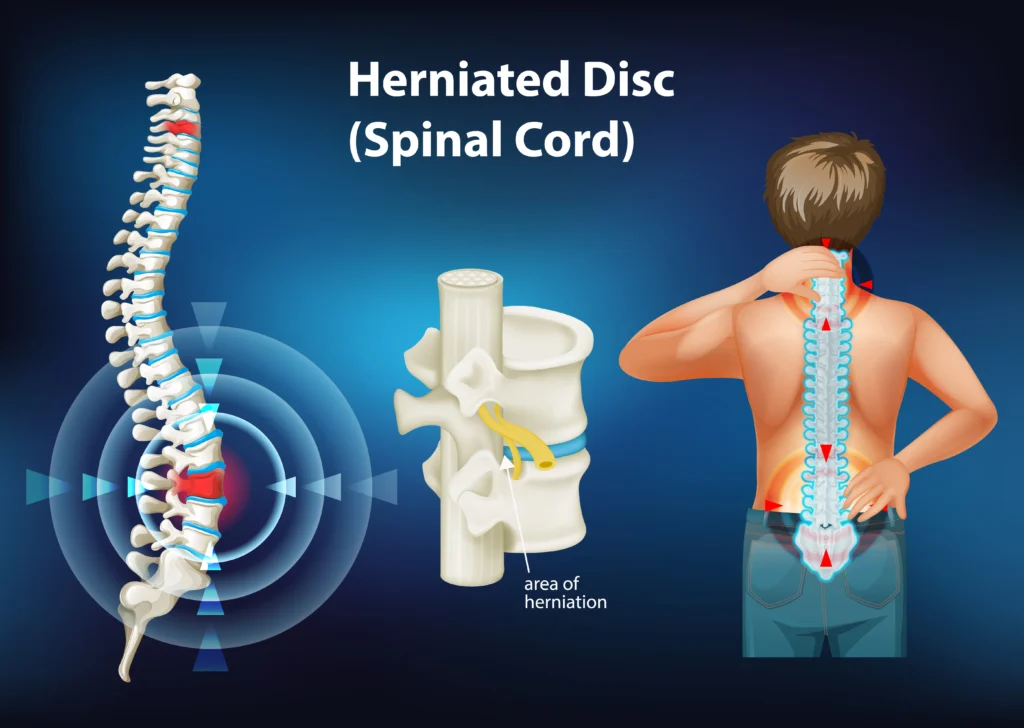
Understanding Your Spine
Think of your spine as a tall stack of building blocks.
Between every two vertebrae sits an intervertebral disc, which works like a shock absorber.
Each disc has two important parts:
- A strong outer ring called the annulus fibrosus
- A soft gel-like center called the nucleus pulposus
Together, they cushion the spine every time you bend, walk, jump, lift, or twist.
Over time, aging, repetitive stress, poor lifting mechanics, smoking, genetics, obesity, and prolonged sitting gradually weaken these discs.
Eventually, the disc may begin to bulge or even rupture.
The World Federation of Neurosurgical Societies notes that lumbar disc herniation most commonly affects adults aged 30 to 50 years and that both genetic and lifestyle factors contribute to disc degeneration. (PubMed)
What Is a Bulging Disc?
A bulging disc occurs when the entire disc extends beyond its normal boundary without breaking its tough outer covering.
Imagine squeezing a jelly-filled doughnut gently.
The doughnut becomes wider, but no jelly leaks out.
That is essentially what happens in a bulging disc.
The disc remains intact, but it protrudes slightly into the spinal canal.
Many bulging discs are considered part of the normal aging process and never cause pain.
Lesser-Known Fact
Research has found that disc bulges are extremely common even among people who have no symptoms whatsoever.
This is why doctors should never recommend surgery solely because an MRI shows a bulging disc.
Clinical examination remains essential. (NCBI)
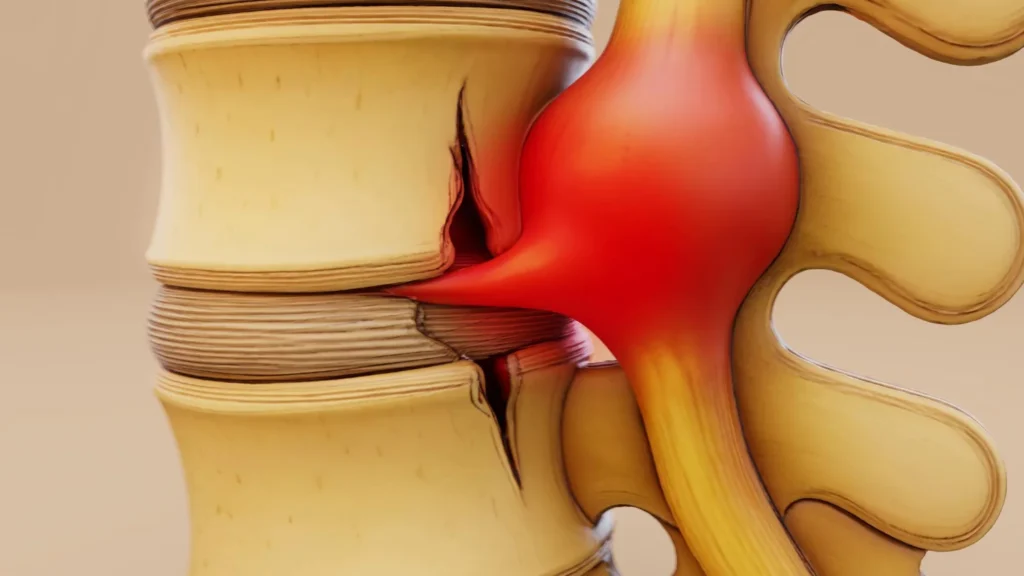
What Is a Herniated Disc?
A herniated disc is more severe.
Here, the outer annulus develops a tear, allowing some of the inner gel-like nucleus pulposus to push outward.
If this leaked material touches or compresses a nearby spinal nerve, symptoms can become much more noticeable.
People often experience:
Interestingly, the size of the herniation does not always predict the severity of symptoms.
A relatively small herniation in the wrong location may produce severe nerve pain, while a larger one elsewhere may remain painless. (PMC)
Bulging Disc vs Herniated Disc: The Simplest Way to Remember
Imagine a balloon filled with toothpaste.
Bulging Disc
The balloon expands outward.
Nothing leaks.
The wall stays intact.
Herniated Disc
The balloon develops a small hole.
Some toothpaste escapes.
That escaped material may press directly on nearby nerves.
This simple comparison helps explain why herniated discs are generally more likely to cause nerve-related symptoms.
Can a Bulging Disc Turn Into a Herniated Disc?
Yes.
Not every bulging disc progresses to a herniation, but some do.
Repeated bending under heavy loads, poor lifting techniques, smoking, obesity, and ongoing degeneration may weaken the outer annulus further until it eventually tears.
The good news is that progression is not inevitable.
Maintaining a healthy body weight, improving core strength, practicing proper lifting mechanics, staying physically active, and following a structured physiotherapy program;
can reduce mechanical stress on the spine.
Evidence also suggests that conservative management, including physiotherapy, provides meaningful symptom relief for many patients with lumbar disc herniation and radicular pain. (Felix De Bruyn et al., PMC)
Why MRI Reports Often Scare Patients Unnecessarily
One of the biggest misconceptions is believing that an MRI diagnosis automatically explains your pain.
In reality, MRI findings are only one piece of the puzzle.
Your healthcare provider should consider:
- Your symptoms
- Pain location
- Muscle strength
- Reflexes
- Walking pattern
- Nerve tension tests
- Functional limitations
Recent treatment guidelines emphasize that clinical examination should guide management decisions, and imaging findings alone should not dictate treatment. (NeuroSpine)
Bulging Disc vs Herniated Disc: Side-by-Side Comparison
Although both conditions affect the intervertebral discs, they differ in how much damage has occurred, the symptoms they produce, and how they are managed.
Understanding these differences can help reduce unnecessary anxiety and encourage appropriate treatment decisions.
| Feature | Bulging Disc | Herniated Disc |
|---|---|---|
| Outer disc layer | Intact | Torn or ruptured |
| Inner gel | Remains inside the disc | Pushes through the tear |
| Nerve compression | Less common | More common |
| Pain severity | Often mild or absent | May range from mild to severe |
| Numbness and tingling | Uncommon | Common if a nerve is compressed |
| Muscle weakness | Rare | Possible |
| MRI appearance | Broad-based disc protrusion | Localized disc extrusion or protrusion |
| Surgery needed | Rarely | Occasionally, if conservative treatment fails or neurological deficits develop |
Research shows that the majority of lumbar disc conditions improve with conservative treatment, and only a small percentage eventually require surgery. (BMJ)
Symptoms of a Bulging Disc
One of the biggest surprises for many patients is that most bulging discs never cause pain.
A bulging disc may simply be an age-related change discovered during an MRI performed for another reason.
However, if the bulge becomes large enough to narrow the spinal canal or irritate a nearby nerve, symptoms can include:
- Localized back pain
- Neck stiffness
- Mild aching after prolonged sitting
- Pain during bending
- Reduced spinal flexibility
- Occasional muscle tightness
Symptoms often fluctuate throughout the day and may improve with gentle movement.
Symptoms of a Herniated Disc
A herniated disc is more likely to produce nerve-related symptoms;
because the escaped disc material contains inflammatory chemicals that can irritate spinal nerves in addition to mechanically compressing them.
Typical symptoms include:
- Sharp back pain
- Sciatica
- Neck pain radiating into the arm
- Burning pain
- Tingling
- Pins and needles
- Numbness
- Muscle weakness
- Difficulty walking
- Pain while coughing or sneezing
Interestingly, inflammation often contributes as much to pain as physical pressure on the nerve.
This explains why symptoms sometimes improve even before the herniated material significantly shrinks. (Life Fit Wellness)
Does the Size of the Herniation Matter?
Many people assume:
“Bigger herniation equals worse pain.”
That is not always true.
I’ve treated patients with very large herniated discs who experienced only mild discomfort, while others with relatively small herniations suffered severe sciatica.
Pain depends on several factors:
- Location of the herniation
- Degree of nerve inflammation
- Individual pain sensitivity
- Presence of muscle spasm
- Existing spinal degeneration
This is why MRI findings should always be interpreted together with a detailed physical examination.
Lesser-Known Fact: Your Body Can Remove a Herniated Disc Naturally
One fascinating discovery over the past two decades is that the body is capable of reabsorbing herniated disc material.
Special immune cells called macrophages gradually break down and remove the extruded disc fragments.
This natural healing process explains why many patients improve significantly over several months without surgery.
Several systematic reviews have demonstrated spontaneous regression of lumbar disc herniations, especially larger extrusions and sequestrations. (MDPI)
As physiotherapists, this knowledge allows us to reassure patients that healing is possible with time, movement, and guided rehabilitation.
Can a Bulging Disc Heal?
This is one of the most common questions I hear.
Technically, the disc itself rarely returns completely to its original shape.
However, symptoms often improve because:
- Inflammation settles
- Muscles become stronger
- The spine moves more efficiently
- Nearby tissues adapt
- The nervous system becomes less sensitive
Many people become completely pain-free even though their MRI continues to show a bulging disc.
The goal of treatment is not necessarily to create a “perfect MRI” but to restore pain-free function and confidence in movement.
Can a Herniated Disc Heal?
Yes.
Contrary to popular belief, most herniated discs improve without surgery.
Clinical guidelines recommend conservative treatment as the first-line approach for patients without serious neurological deficits.
Recovery usually involves:
- Physiotherapy
- Activity modification
- Walking
- Pain management
- Progressive strengthening
- Education about safe movement
The timeline varies from person to person, but many patients experience substantial improvement within 6 to 12 weeks, while continued healing can occur over several months. (MMPT)
Why Physiotherapy Is Often More Important Than Rest
Years ago, prolonged bed rest was commonly recommended for disc problems.
Today we know that excessive rest may actually delay recovery.
Remaining inactive can lead to:
- Muscle weakness
- Joint stiffness
- Reduced circulation
- Increased fear of movement
- Slower recovery
Modern physiotherapy focuses on restoring normal movement while avoiding unnecessary strain on the healing tissues.
Research consistently supports exercise-based rehabilitation for improving pain, disability, and function in people with lumbar disc disorders. (NLM)
Bulging Disc vs Herniated Disc: A Physiotherapist’s Approach to Treatment
Every patient is different.
Rather than treating MRI findings, I focus on identifying the movements that provoke symptoms and gradually restoring tolerance to those activities.
Treatment may include:
Pain Management
- Activity modification
- Heat or ice when appropriate
- Manual therapy in selected patients
- Gentle mobility exercises
Improving Mobility
Restricted hips and stiff thoracic spines often increase stress on the lumbar discs.
Improving movement in these areas may reduce pressure on the lower back.
Core Strengthening
A stronger core improves spinal stability without making the back rigid.
Exercises may include:
- Abdominal bracing
- Bird Dog
- Dead Bug
- Modified side plank
- Pelvic tilts
Progression should always be individualized rather than rushed.
Nerve Mobility Exercises
If nerve irritation is present, carefully prescribed nerve gliding exercises may help reduce sensitivity.
These should be performed under professional guidance because excessive stretching can worsen symptoms.
Daily Habits That Help Recovery
Small lifestyle changes often have a bigger impact than people expect.
I encourage my patients to:
- Walk several times each day.
- Change sitting position every 30 to 45 minutes.
- Lift with the hips and knees rather than bending through the spine.
- Sleep on a supportive mattress.
- Maintain a healthy body weight.
- Stay hydrated.
- Continue gentle daily activities whenever possible.
- Consistency matters more than intensity.
Things to Avoid During Recovery
Many setbacks occur because patients unknowingly overload healing tissues.
Try to avoid:
- Prolonged bed rest
- Heavy lifting with a rounded back
- Sudden twisting while carrying weight
- Smoking, which reduces blood supply to spinal tissues
- Ignoring persistent numbness or weakness
- Returning to intense exercise too quickly
- Sitting continuously for several hours
These habits increase mechanical stress and may delay recovery.
Lesser-Known Fact: Smoking Affects Disc Health
Most people know smoking harms the lungs and heart.
Far fewer realize that smoking also accelerates disc degeneration.
Nicotine reduces blood flow to spinal structures, limiting the delivery of oxygen and nutrients that help maintain healthy discs.
Smokers are more likely to develop degenerative disc disease and experience poorer healing after spine injuries and surgery. (Spine; Phila Pa 1976)
When Is Surgery Actually Necessary?
One of the biggest misconceptions I hear in the clinic is:
“My MRI shows a herniated disc, so I probably need surgery.”
Fortunately, that is rarely true.
Current international guidelines recommend conservative management as the first-line treatment for most people with lumbar disc herniation,
provided there are no serious neurological deficits or emergency symptoms.
Physiotherapy, activity modification, pain management, and gradual exercise help the majority of patients recover without an operation. (PMC)
Surgery may be considered if:
- Severe leg or arm pain persists despite several weeks of appropriate conservative treatment.
- Progressive muscle weakness develops.
- Daily activities remain significantly limited despite rehabilitation.
- MRI findings match the patient’s symptoms and physical examination.
- Emergency neurological symptoms develop.
Remember, the goal is to treat the patient, not the MRI.
Red Flag Symptoms That Require Immediate Medical Attention
Although most bulging and herniated discs are not emergencies, some symptoms require urgent medical evaluation.
Seek immediate medical care if you experience:
- Loss of bladder or bowel control
- Numbness around the groin or inner thighs (saddle anesthesia)
- Rapidly worsening leg or arm weakness
- Difficulty walking because of increasing weakness
- Severe pain following major trauma
- Fever, unexplained weight loss, or history of cancer with new back pain
These symptoms may indicate cauda equina syndrome, spinal infection, fracture, or another serious condition, where early treatment is critical. (Cleveland Clinic)
Things You Should Do Every Day
As a physiotherapist, I often tell patients that recovery is influenced more by daily habits than by occasional treatment sessions.
Stay Active
Gentle walking encourages circulation, reduces stiffness, and helps restore confidence in movement.
Strengthen Your Core
A strong core acts like a natural support system for the spine without making it rigid.
Improve Hip Mobility
Stiff hips often force the lower back to move excessively during bending and lifting.
Practice Proper Lifting Mechanics
- Bend at your hips and knees.
- Keep the object close to your body.
- Avoid twisting while lifting.
Take Frequent Movement Breaks
If your job involves prolonged sitting, stand up and move every 30-45 minutes.
Maintain a Healthy Weight
Excess body weight increases mechanical stress on spinal discs and may accelerate degeneration. (NCBI)
Things to Avoid
Recovery is often delayed by repeated mechanical irritation.
Try to avoid:
- Sitting continuously for several hours
- Heavy lifting with a rounded back
- Repeated twisting under load
- Smoking
- High-impact exercise during acute flare-ups
- Ignoring progressive weakness or numbness
- Staying in bed for days
Modern evidence strongly discourages prolonged bed rest because it contributes to muscle weakness, reduced function, and slower recovery. (Biomed Central)
Lesser-Known Facts About Disc Problems
Your MRI May Never Become “Normal”
Even after your symptoms disappear, your MRI may continue to show a disc bulge or herniation.
Pain relief often occurs because inflammation settles, muscles become stronger, and the nervous system becomes less sensitive,
not necessarily because the disc returns to its original shape. (Spine Surgery and Related Research)
Bigger Herniations Often Shrink More
This surprises many patients.
Research suggests that extruded and sequestrated herniations are actually more likely to undergo spontaneous resorption than small contained bulges because they trigger a stronger immune response. (J Neurosurg Spine . 2023 )
Many Healthy Adults Have Disc Bulges
MRI findings do not always explain pain.
Disc bulges and other degenerative changes are frequently seen in people who have no back pain at all, especially as they age.
This is why imaging should always be interpreted alongside a detailed clinical examination.
Myth vs Reality
| Myth | Reality |
|---|---|
| Every bulging disc causes pain. | Many bulging discs are completely painless. |
| Herniated discs always require surgery. | Most improve with conservative care. |
| Complete bed rest is the best treatment. | Gentle movement and physiotherapy are generally recommended. |
| A larger herniation always causes worse symptoms. | Pain depends more on nerve involvement than disc size. |
| MRI findings alone determine treatment. | Symptoms and physical examination are equally important. |
Clinical Insight
One lesson I’ve learned from treating patients with spinal disorders is that fear often causes more disability than the disc itself.
Many people stop walking, exercising, travelling, or even picking up their children because they believe their spine has become fragile.
In reality, the spine is remarkably adaptable.
A structured rehabilitation program, progressive strengthening, and patient education can restore confidence and function for many individuals.
Your MRI is just one part of the story; your symptoms, goals, and overall health matter just as much.
Physio Prescription
If you have been diagnosed with a bulging or herniated disc:
- Walk every day within your pain tolerance.
- Perform your prescribed physiotherapy exercises consistently.
- Avoid prolonged sitting.
- Build core and hip strength gradually.
- Practice proper posture and lifting techniques.
- Sleep adequately to support tissue recovery.
- Stay patient—healing often takes weeks to months.
Small, consistent improvements usually produce better long-term outcomes than aggressive treatment.
Final Word
A bulging disc vs herniated disc are not the same condition, even though the terms are often confused.
A bulging disc involves an outward extension of the disc while the outer layer remains intact.
A herniated disc occurs when that outer layer tears and the inner material escapes, making nerve irritation more likely.
The encouraging news is that most people improve without surgery.
Evidence supports a conservative approach that includes physiotherapy, education, appropriate exercise, and lifestyle modifications for the majority of patients.
Surgery is generally reserved for those with persistent disabling symptoms or significant neurological deficits.
Rather than focusing solely on what your MRI says, focus on what your body can do today and take steady steps toward better movement, strength, and confidence.
Frequently Asked Questions
1. Is a bulging disc the same as a herniated disc?
No. A bulging disc occurs when the disc extends outward but its outer layer remains intact. A herniated disc develops when the outer layer tears, allowing the soft inner material to push out and potentially compress nearby spinal nerves.
2. Which is more painful, a bulging disc or a herniated disc?
Herniated discs are generally more likely to cause severe pain because they can irritate or compress spinal nerves. However, pain depends more on the location of the disc problem than its size.
3. Can a bulging disc turn into a herniated disc?
Yes. Continued degeneration, poor lifting mechanics, repetitive strain, obesity, and smoking may increase the risk of a bulging disc progressing to a herniated disc, although many bulging discs never worsen.
4. Can a herniated disc heal without surgery?
Yes. Most herniated discs improve with physiotherapy, exercise, activity modification, pain management, and time. Surgery is usually reserved for persistent symptoms or significant nerve damage.
5. Does every bulging disc cause symptoms?
No. Many people have bulging discs visible on MRI scans without experiencing any pain or neurological symptoms.
6. Is walking good for a bulging or herniated disc?
In most cases, yes. Gentle walking promotes circulation, reduces stiffness, and supports recovery. However, walking should be comfortable and guided by your physiotherapist if symptoms worsen.
7. How long does it take for a bulging or herniated disc to recover?
Many patients notice improvement within 6 to 12 weeks, although complete recovery may take several months depending on the severity, lifestyle, and adherence to rehabilitation.
8. What activities should I avoid with a herniated disc?
Avoid heavy lifting with a rounded back, repetitive twisting, prolonged sitting, high-impact activities during flare-ups, and smoking, as these may delay healing.
9. Can physiotherapy help both bulging and herniated discs?
Yes. Physiotherapy is considered a first-line treatment for most disc conditions. It focuses on reducing pain, improving mobility, strengthening the core, restoring movement, and preventing future recurrences.
10. When should I seek emergency medical attention for a disc problem?
Seek immediate medical care if you develop loss of bladder or bowel control, numbness around the groin, rapidly worsening weakness, or severe symptoms following significant trauma.
Stay tuned with us for more health related topics.
Follow us on LinkedIn and Instagram for more.
More Read






Medical Disclaimer!
This article has been reviewed and written under the guidance of our Head Physiotherapist, Dr. Kruti Raj (PT, MUHS,CPT,CMPT). The information shared is intended for educational purposes only and should not be considered a substitute for personalized medical advice, diagnosis, or treatment.
Please consult us or any other qualified healthcare professional before beginning any exercise program, especially if you are experiencing pain, recovering from injury, or managing a medical condition.



